
alternative care models top tips
VACANCIES VS APPLICANTS
Are vacancies and soaring contract labor rates causing you to reevaluate your patient care delivery models? You have more options than you may think!
FOUR EXAMPLES
When short on RNs, what are your options to maintain your standard of care? The answer may be different – even among nursing units in the same hospital.
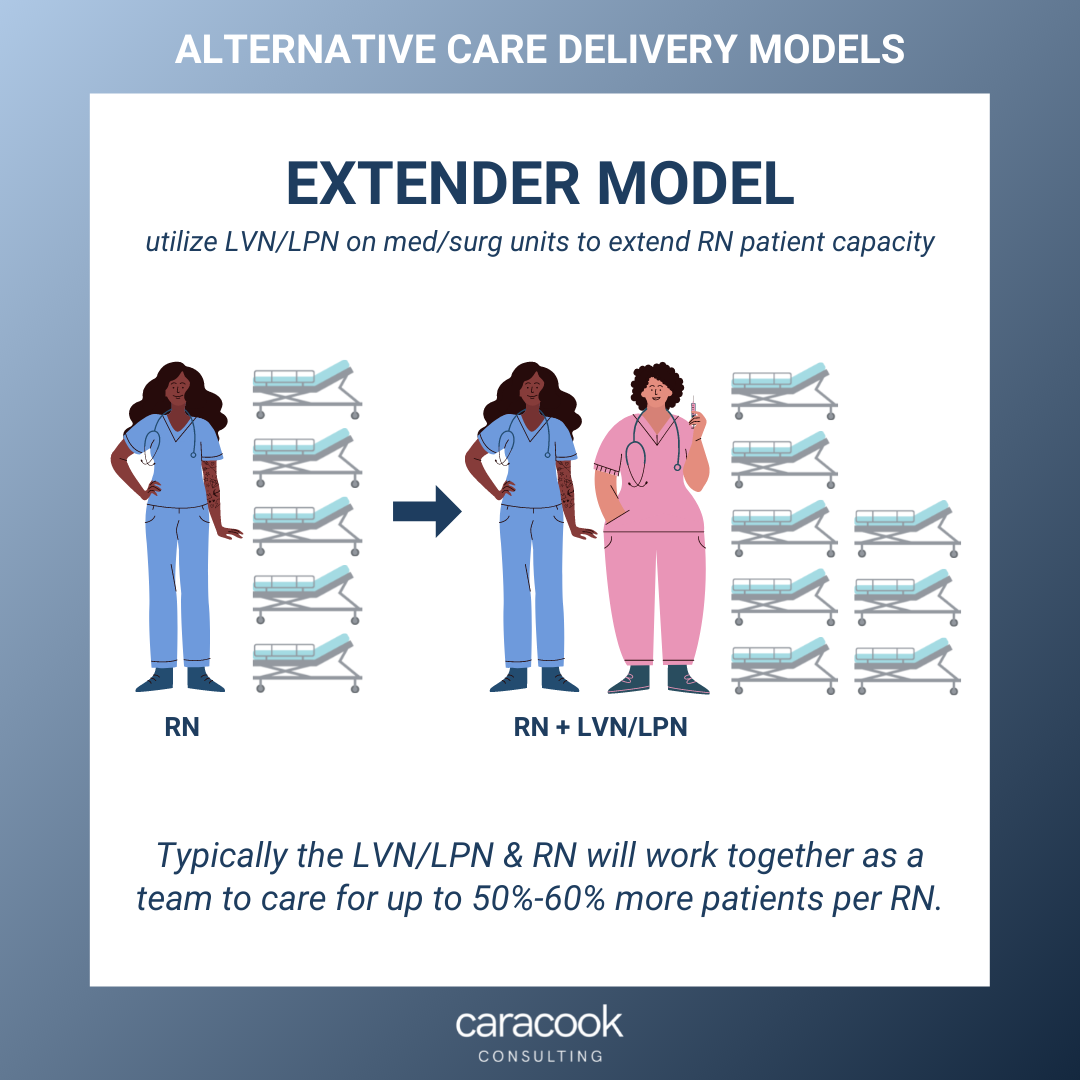
EXTENDER MODEL
The extender model utilizes LVN/LPN on Med/Surg units to extend RN patient capacity. Typically the LVN/LPN & RN will work together as a team to take 50%-60% more patients per RN. For example, if your current Med/Surg ratio is 1 RN to 5 patients, your extender team could take anywhere between 7 to 8 patients depending on acuity.
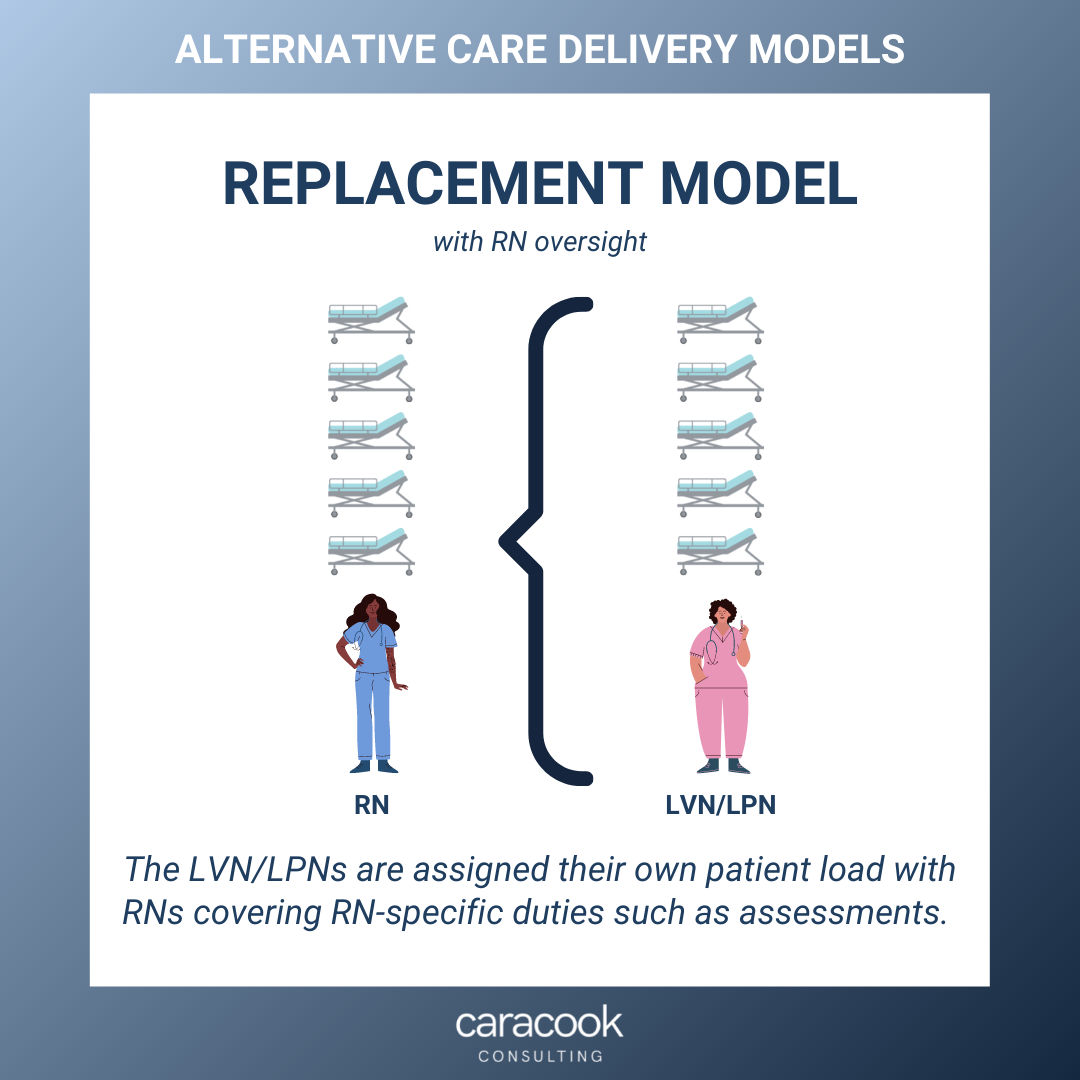
REPLACEMENT MODEL
In the replacement model, the LVN/LPNs will take their own patient load with RNs assigned to cover RN scope of practice duties such as assessments. The RNs will take patient assignment of their own but oversee RN duties for assigned LVNs.
IN PLACE OF TECHS
Some med/surg and intermediate units are able to increase RN ratios slightly when using higher functioning LVN/LPNs instead of techs. Depending on size of the unit, some techs may support patient bathing, stocking, and other specific duties while the others are replaced with LVN/LPNs to provide nursing support for RNs.
TEAM MODEL
The team model is the most popular. It is especially efficient for units with census levels that correspond to the patient ratios per team. In the team model, a team of 1 RN, 1 LVN/LPN, & 1 PCA/Tech take a group of patients. For a med/surg unit the patient assignment size would be 10-12. The RN leads the team and coordinates care between the team members. This model lends well to each staff member working at the highest level of licensure.